Advanced Bronchoscopy Services
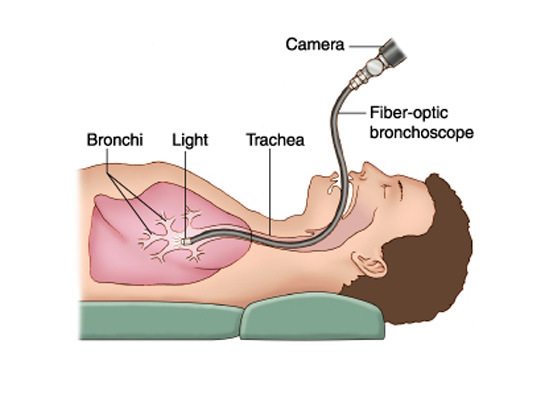
Bronchoscopy is a technique of visualizing the inside of the airways for diagnostic and therapeutic purposes. An instrument (bronchoscope) is inserted into the airways, usually through the nose or mouth, or occasionally through a tracheostomy. This allows the practitioner to examine the patient's airways for abnormalities such as foreign bodies, bleeding, tumors, or inflammation. Specimens may be taken from inside the lungs. The construction of bronchoscopes ranges from rigid metal tubes with attached lighting devices to flexible optical fiber instruments with real-time video equipment.
Rigid bronchoscopy is used for retrieving foreign objects. Massive hemoptysis, defined as loss of >600 mL of blood in 24 hours, is a medical emergency and should be addressed with initiation of intravenous fluids and examination with rigid bronchoscopy. The larger lumen of the rigid bronchoscope versus the narrow lumen of the flexible bronchoscope allows for therapeutic approaches such as electrocautery to help control the bleeding. Rigid bronchoscopy is preferred for recovery of foreign body aspiration because it allows protection of the airway and controlling the foreign body during recovery.
A flexible bronchoscope is longer and thinner than a rigid bronchoscope. It contains a fiberoptic system that transmits an image from the tip of the instrument to an eyepiece or video camera at the opposite end. Using Bowden cables connected to a lever at the hand piece, the tip of the instrument can be oriented, allowing the practitioner to navigate the instrument into individual lobe or segment bronchi.
Most flexible bronchoscopes also include a channel for suctioning or instrumentation, but these are significantly smaller than those in a rigid bronchoscope.Flexible bronchoscopy causes less discomfort for the patient than rigid bronchoscopy and the procedure can be performed easily and safely under moderate sedation. It is the technique of choice nowadays for most bronchoscopic procedures.
EndoSheath® Bronchoscopy is a new alternative to conventional Bronchoscopy procedures.For the first time, Pulmonologists and Bronchoscopists can get high performance endoscopic imaging and functionality with the EndoSheath® Technology, the only sterile, disposable option for flexible endoscopy.The BRS-5000 Bronchoscope is the only flexible video bronchoscope that never comes in contact with the patient. The EndoSheath® Technology provides a durable, protective barrier, as well as a disposable working channel. All patient materials and instrumentation from biopsy tissue samples to BAL fluid removal, travel through the channel in the disposable sheath and never come in contact with the reusable bronchoscope.
The Pediatric Flexible Bronchoscopy is available for the diagnosis and treatment of a number of pediatric airway conditions. This procedure allows physicians to perform a direct visual examination of the vocal cords, upper airways and lungs. Common conditions investigated include those associated with noisy breathing and stridor, such as laryngomalacia, tracheobronchomalacia, and narrowing of the subglottic space. Flexible bronchoscopy is used for the work-up of recurrent pneumonia, persistent non-asthmatic wheezing, suspected airway compression, chronic cough, and suspected foreign body.
The small size of the child's airway, differences in the anatomy of the larynx and the different pathologies according to age group, are characteristics that shows the endoscopic examination of the child quite unique and different from adults. The infant larynx presents some different aspects compared to the adult. Its location is higher in the neck, the cricoid cartilage being located approximately at the fourth cervical vertebra. With the growth of the child the cricoid cartilage will gradually descend to the level of the seventh cervical vertebra, which is the location in adulthood. The size of the larynx in the newborn is about 1 / 3 of the adult. Their structures such as the vocal process of arytenoid, cuneiform cartilage, the arytenoids and the soft tissue that makes up the supraglottic larynx are also bigger. The epiglottis is proportionally more posterior and narrower and more tubular or omega-shaped